 For insurance carriers, relationships have historically focused on three key stakeholders: rate payers, brokers and clinicians. Commercial carriers have moved from being primarily fiduciary intermediaries to playing a more pivotal role in the health and lives of members. It is no longer sufficient to simply identify the best providers for the population, underwrite risk and pay for care.
For insurance carriers, relationships have historically focused on three key stakeholders: rate payers, brokers and clinicians. Commercial carriers have moved from being primarily fiduciary intermediaries to playing a more pivotal role in the health and lives of members. It is no longer sufficient to simply identify the best providers for the population, underwrite risk and pay for care.
We have taken on new, innovative roles, including:
- Ensuring that evidence-based medicine is practiced.
- Providing guidance for managing the delivery system.
- Identifying gaps in care for members and their providers.
- Providing incentives to clinicians and hospitals for improving health outcomes.
This transformation has been driven by the realization that health outcomes in the United States were not improving at the same pace as costs were rising. It has become clear that we as Americans created the system that ate the economy! While these improvements have begun to move the needle on improved quality, better outcomes and slowing the rate of inflation, these improvements were still not meeting the needs of the population.
Within the Medicaid program, these challenges have been even more acute. Managed Medicaid has significantly improved the cost of medical care for our most vulnerable citizens and has made key differences in outcomes. At United, we’ve moved to a more comprehensive approach. We have:
- Expanded the role of call center representatives to an “advocate for me.” They not only answer questions, but facilitate resolutions outside of the health plan.
- Made extensive use of Community Health workers who conduct outreach within the community in support of managing more complex situations.
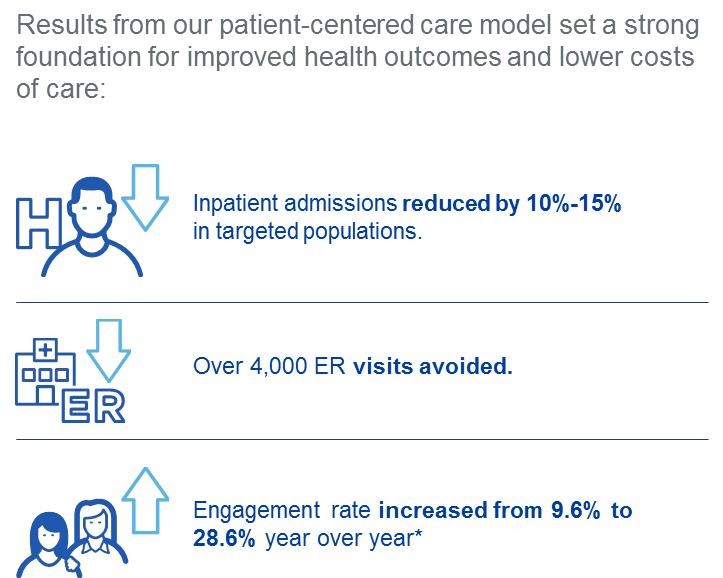
- Created Accountable Care Organizations and patient-centered models of care to close gaps in care and ensure follow-up with primary care clinicians after hospital stays and ER visits.
- Supported these improvements with comprehensive incentives for primary care clinicians. In the first half of 2016, we paid clinicians over $3.2 million in quality and cost payments in Louisiana alone.
- Integrated behavioral health within the medical plan to address care issues for which the lines are blurred.
The programs outlined above point to a more personalized approach to medical care that is paying dividends, sourced in this 2015 United whitepaper.
Our experience has shown that today’s Medicaid populations include an increasing number of individuals with behavioral health diagnoses and social service needs, in addition to existing chronic health conditions. To effectively serve the needs and improve the health of these populations, we must address the whole person.
At United, “Whole Person Care” is the next frontier in health care. Our data analytics have shown:
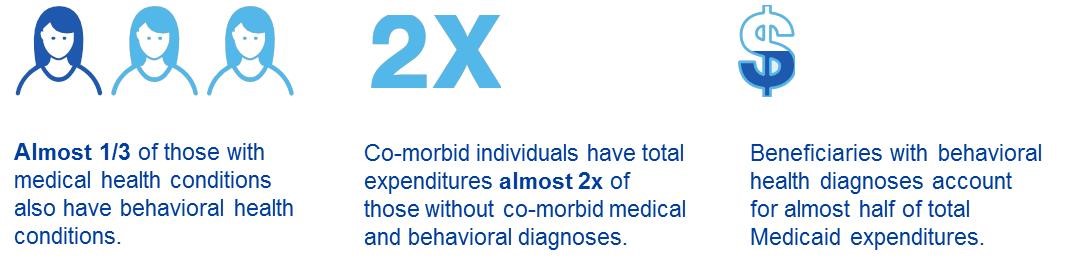
Given the factors outlined above, the model of care for our most challenging situations warrants a more comprehensive and innovative approach. By moving beyond the “medical home” we take the time to understand and address the psycho-social issues that have impeded the effectiveness of the most advanced medical treatments. Whole-person care enables us to understand the challenges faced by members not only in managing health, but in managing their lives. We believe that this added dimension will enable the medical/behavioral/community teams to engage members in unprecedented ways and resolve issues that in the past were overlooked. Our approach to whole-person care is illustrated as follows
Addressing the whole person

Under this model we take into account the social determinants of health. We firmly believe that integrating social determinants and behavioral health with medical care has the potential for significantly improved outcomes for the Medicaid population. We are excited about the potential for this new approach to comprehensive health care. Tune in next year to hear about our results!